Schulze Surgery Center Celebrates Its 20 Year Anniversary!
We are happy to announce that February, 2017 marks our 20th consecutive year of operation. In the 1990’s, Dr. Schulze Jr & Sr recognized the need for a venue for affordable, convenient, and high quality surgery for our cataract and refractive surgery patients.
Prior to that time, all eye surgeries were performed in the hospital, and while quality was good, the size and bureaucracy of the hospitals did not lend themselves to efficiency, and costs to the patient were roughly double (and, in some documented cases, up to ten times as high) what was spent on facility fees in the ambulatory surgery center setting. Although Dr. Schulze, Sr. had long wanted to build a surgery center, Georgia state law prevented him from doing so, mainly because the powerful hospital lobby was against any competition for their services. After all, they had a government sponsored monopoly on surgery, and could essentially charge whatever they wanted for their services.
But the laws changed in the mid ’90’s, and Dr. Schulze, Jr and Sr teamed up to build the first outpatient surgery center specializing in eye surgery in coastal Georgia. Construction took place in 1996, and we opened our doors for our first surgeries in 1997. Since that time, we’ve had the opportunity to serve tens of thousands of #cataract and #LASIK patients, saving our patient base millions of dollars in the process as compared to what they would have spent in the hospital setting. More importantly, however, we have been able to provide first class care to an entire generation of patients, and we look forward to carrying on these traditions of quality and innovation for generations to come.
The Symfony Lens: Enhanced Optics for the Active Lifestyle after Cataract Surgery
The Holy Grail for eye surgeons would be to have an implant that would provide for simultaneous far and near vision–and everything between–after cataract surgery. Although multifocal intraocular lenses have been in common use now for over 20 years, they are not for everyone. Specifically, certain conditions such as astigmatism, retinal or corneal disease, and dry eye can make vision after multifocal implants less than optimal.
Last year, the Symfony intraocular lens, made by AMO, was approved by the FDA. This is the first so called extended depth of focus lens to enter the marketplace, creating a longer range of clear vision as compared to previous multifocal designs through improved optics which correct not only spherical aberration, but also chromatic aberration. Although Symfony patients might not be able to read the very smallest lines of print after surgery, we are finding that they tend to have a more effective range of vision than traditional multifocal IOl patients. Specifically, we’re finding that Symfony patients tend to excel without glasses in real world situations like seeing the dashboard while driving a car and reading a cell phone, tablet, or computer screen, whereas older designs that had more magnification at near tended not to see well with intermediate tasks.
Moreover, the Symfony lens is now available in a toric version that corrects for astigmatism at the same time as it corrects far and near vision. This enables patients who previously were not candidates for multifocal lenses to have an extended range of vision.
Is the Symfony lens the Holy Grail for cataract surgery? Well maybe not quite, but it appears to be the closest thing to it we have at our disposal today. The smiles and happy faces I see the day after surgery, with patients asking, “can I have my second eye done tomorrow” appear to be proof that this technology works.
The EpiPen Fiasco: Why did this happen?
What is a WaveScan?
A WaveScan is a computerized device that we use to create a “fingerprint” of your vision prior to having surgery with LASIK or PRK with the AMO/VISX Star S4 IR excimer laser. Although other people may have the same refraction as you, your WaveScan is unique to you. This technology allows us to capture your refraction, including higher order aberrations, and to upload your diagnostic data to the computer that drives the laser. Because the laser has iris recognition technology (called “iris registration” or “IR”), the laser will know the difference between your right and left eye (thus eliminating the possibility of wrong site surgery) and, after locking onto your eye, will deliver a customized treatment in the exact spot where the diagnostic data were acquired.
Carrying on our tradition of innovation in eye surgery, the Schulze Surgery Center was the first center in coastal Georgia to offer this technology. Using the WaveScan together with our AMO/VISX Star S4 IR excimer laser allows us to offer truly customized wavefront guided LASIK and PRK, called CustomVue.
Data submitted to the FDA for CustomVue LASIK found the following:
- 4x as many participants in the low to moderate myopia clinical study were very satisfied with their night vision after the Advanced CustomVue Procedure, compared to their night vision before with glasses or contact lenses
- 4x as many participants in the hyperopia clinical study were very satisfied with their night vision after the Advanced CustomVue Procedure, compared to their night vision before with glasses or contact lenses
- Nearly 2x as many participants in the mixed astigmatism clinical study were very satisfied with their night vision after the Advanced CustomVue Procedure, compared to their night vision before with glasses or contact lenses
- 90% of patients surveyed in the high myopia clinical study were more satisfied, or as satisfied with their vision after the Advanced CustomVue Procedure as they were before with glasses or contact lenses
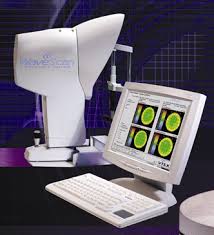
What is LASIK?
LASIK is an acronym for “laser assisted in situ keratomileusis.” The procedure uses the excimer laser to reshape the cornea so as to correct your nearsightedness, farsightedness, and astigmatism. With LASIK, the laser reshapes the cornea underneath a corneal flap (think of the flap as being like a trap door on the surface of the cornea) allowing for quicker healing with less pain. In fact, most of our LASIK patients are back to their normal activities the day after surgery.
Our practice began performing LASIK back in 1997. Not everyone is a candidate for LASIK, but for those who aren’t, we also perform other refractive procedures such as the ICL and Refractive Lens Exchange
- 1
- 2