A magna cum laude graduate of Princeton University, Dr. Schulze went on to study English literature at Oxford University, receiving his M. Phil. degree, before graduating with his M.D. from the University of Virginia in 1990. He performed his internship at Roanoke Memorial Hospital in Virginia before moving on to his residency in ophthalmology at the Ochsner Clinic in New Orleans.
After a year of fellowship training in anterior segment surgery of the eye at the Kentucky Eye Institute, Dr. Schulze, Jr. returned home to Savannah in partnership with his father. Dr. Schulze, Jr. is a member of the American Medical Association, the American Academy of Ophthalmogy, the American Society of Cataract and Refractive Surgery, the International Society of Refractive Surgery, and the Medical Advisory Board of the Georgia Eye Bank.
Dr. Schulze, Jr. specializes in cataract and refractive surgery. Outside of ophthalmology, his interests include windsurfing, sailing, fishing, hunting, farming, and literature.
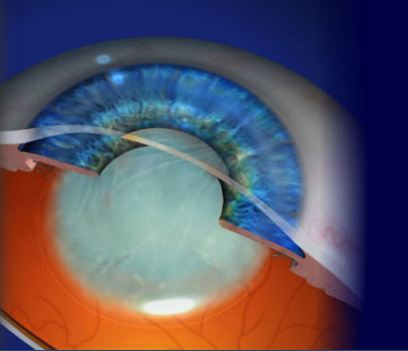
A cataract (from the latin word for “waterfall”) is simply a cloudy lens. You can imagine how a cloudy lens would block light that needs to go through your eye in order to see. What we do with #cataract surgery is quite simple: we take out the cloudy lens and replace it with a clear one. For obvious reasons, you see better through a clear lens than you do through a cloudy one.
Here’s where this gets interesting: understand that when we remove the cloudy lens and replace it with a clear one, we can insert any power lens that we want! Because the techniques for measuring the eye prior to surgery have become so sophisticated, we can now plan our surgery so that nearly all of our patients have less dependence on glasses and contacts, and some patients can even eliminate glasses and contacts entirely.
Take a look at the cataract section on our website here to learn more, and check back for future posts in this blog as we discuss nuances of cataract surgery.
Here’s a little eye surgery trivia for you. This canopy from a British Spitfire fighter plane gave Sir Harold Ridley the idea for the intraocular lens. A fighter pilot in the Second World War was shot down and a fragment of the canopy entered his eye.
Normally, the eye rejects any foreign body with a violent inflammatory immune response. In the case of the fighter pilot, however, the eye remained quiet. Dr Ridley realized he could make clear lenses out of the same material of the canopy and implant these lenses in the eyes of patients who had their natural lens removed with cataract surgery.
Thus was born the intraocular lens (IOL) and, thanks to Dr Ridley’s amazing insight, tens of millions of patients who would otherwise be blind have had their vision restored. Sadly, Dr. Ridley was vilified by the medical establishment during most of his career, and it wasn’t until near the end of his life that his contributions were appreciated.
This is a question I get fairly often from patients coming to me for refractive surgery. Since the excimer laser was first approved for use in 1996, we now have over 20 years of experience to answer this question. Understand that both LASIK and PRK use the same laser, the excimer laser, to reshape your cornea to improve your vision, whether you have nearsightedness, farsightedness, or astigmatism. The difference is that #LASIK reshapes your cornea underneath a flap (think of the flap as being like a trap door on your cornea) whereas #PRK reshapes your eye on the surface.
LASIK offers the advantage of quicker healing. Most patients with LASIK have excellent vision the day after surgery. Disadvantages include a greater incidence of dry eye symptoms and the remote but real risk of a flap complication, including subsequent dislocation of the flap after trauma even years after surgery.
PRK takes a little longer to heal, but offers the advantages of simplicity (there’s no LASIK flap to have a complication with) and less incidence of dry eye symptoms. Most PRK patients have useful vision the day after surgery, but may take up to several weeks to achieve their best vision.
Interestingly, because military personnel are in harm’s way and thus at risk for eye trauma, the military tends to prefer PRK over LASIK so as to avoid the risk of flap dislocation. Studies show that quality of vision between PRK and LASIK are essentially identical, with some studies giving the nod to PRK.
So what is best for you? If you have a thin cornea, a history of dry eye, or abnormal topography, PRK would be your best choice. If there is any question as to suitability for LASIK, we generally prefer PRK because of its greater simplicity. Or, if you’re simply not a LASIK or PRK candidate, the implantable contact (collamer) lens–the ICL https://schulze-eye.com/patient-education/staar-visian-icl-implantable-contact-lens/ –or Refractive Lens Exchange (https://schulze-eye.com/patient-education/refractive-lens-exchange/ ) might be best for you. When you come for your consultation, Dr. Schulze will review your findings and help you make a choice that is best for you.
This is a common question I get in my daily practice. Why is it that when we reach the age of about 40, our near vision tends to slip?
A typical story is that patients will come to us with a history of excellent vision for both far and near earlier in life followed by gradually diminishing near vision in late middle age. As presbyopia worsens, you have to hold objects farther and farther away in order to read, until finally you are no longer able to read without the aid of reading glasses, bifocals, or contact lenses (multifocal or monovision). Lots of patients will say, “Doc, my arms aren’t long enough anymore.”
Why does this happen? Understand that the reason you have excellent vision for both far and near in the early stages of life is because of the elastic properties of the human lens. Being elastic, the lens has the ability to change shape, and hence change focus, for objects both far and near in a seamless fashion through a process called accommodation. You don’t have to think about it; it just happens because of reflexes that are hard wired into your nervous system. As we get older, the lens loses its flexible properties and thus its ability to change shape to focus for far and near. Typically, once the lens loses its elasticity, the eye becomes locked in to a focal point for distance and then you become dependent upon reading glasses and bifocals for near vision.
What can we do to treat presbyopia? The simplest solutions include reading glasses and bifocals. Readers have the virtue of being inexpensive, available universally at any drug store for just a few dollars. Start with a lower power (around +1.25 or +1.50) early in life and understand that every few years you will need to increase the power. There is no right or wrong power; whatever works is the one for you. Realize that higher powers will shorten your working distance and bring things closer to you whereas lower powers will lengthen your working distance and push things farther away. Thus you may want different powers for different tasks; e.g., a higher power for reading close up or a lower power for looking at something farther away like a computer screen.
Surgical corrections for presbyopia are available, although these are not for everyone. The ones that work best depend upon your particular situation and age, and these include LASIK for monovision and Refractive Lens Exchange utilizing either a Multifocal IOL or monovision strategy. Older surgical strategies on the cornea such as LTK (Laser Thermal Keratoplasty) and CK (Conductive Keratoplasty) ultimately proved to be only temporary in effect and have been abandoned. Some newer corneal strategies have recently been developed but these typically improve near vision at the expense of far vision and have yet to be proven. Finally, there are eyedrops for presbyopia under development but there are not yet FDA approved.